Histomorphometry
Number of lobules in biopsy
Number of atrophic lobules
Estimated acinar surface area (mm²)
Acinar Histologic Findings (if adequate sampling)
Qualifiers
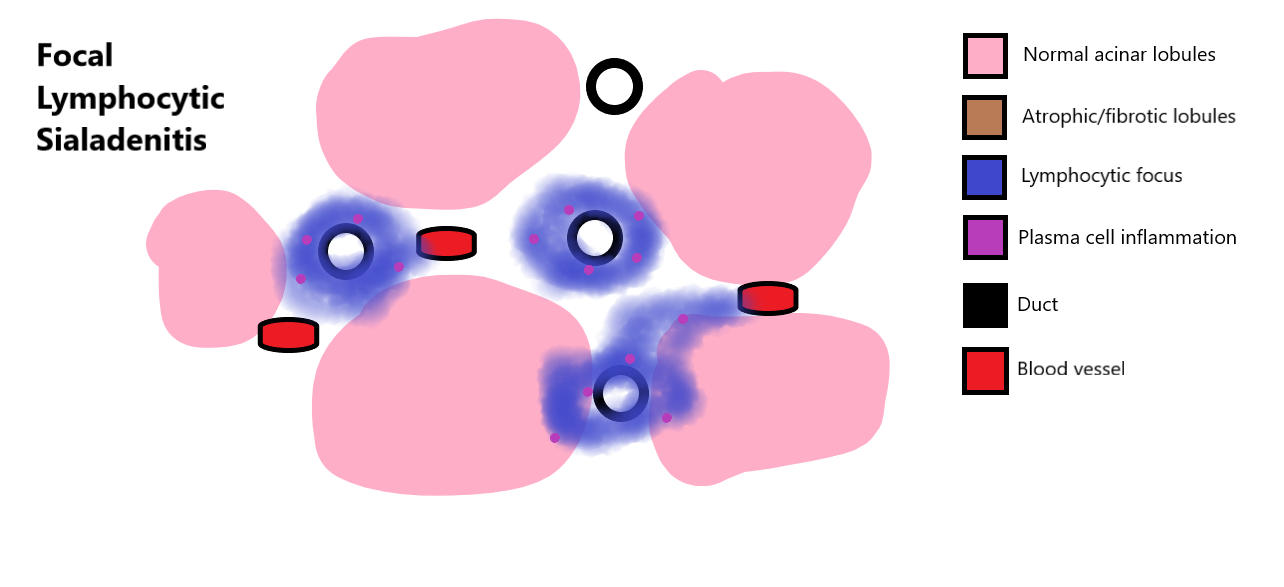
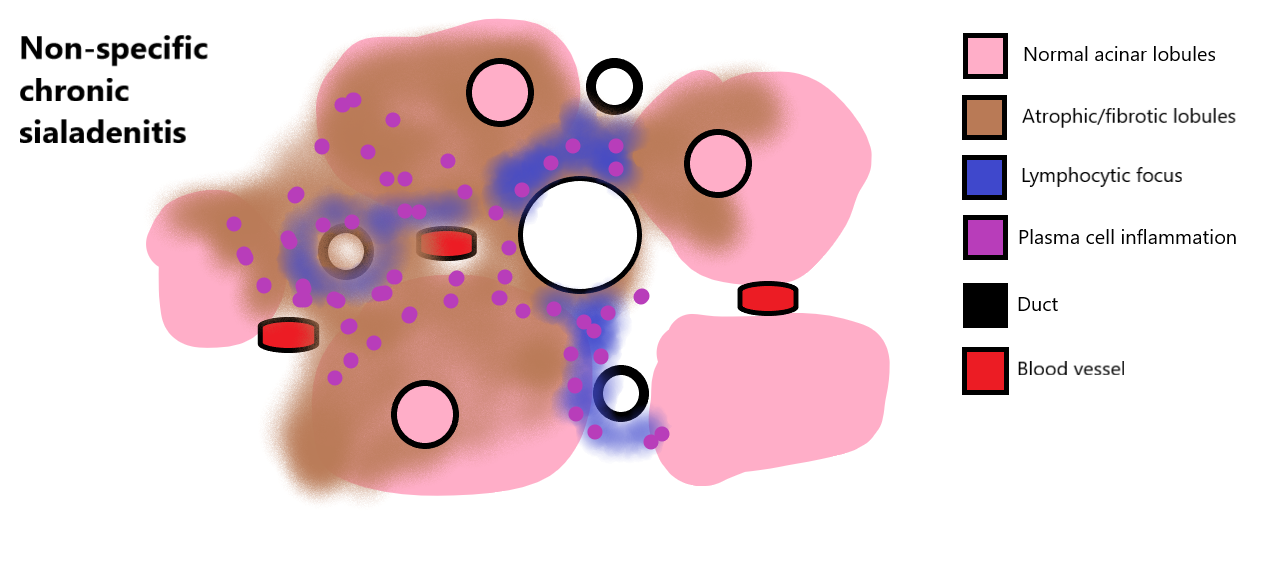
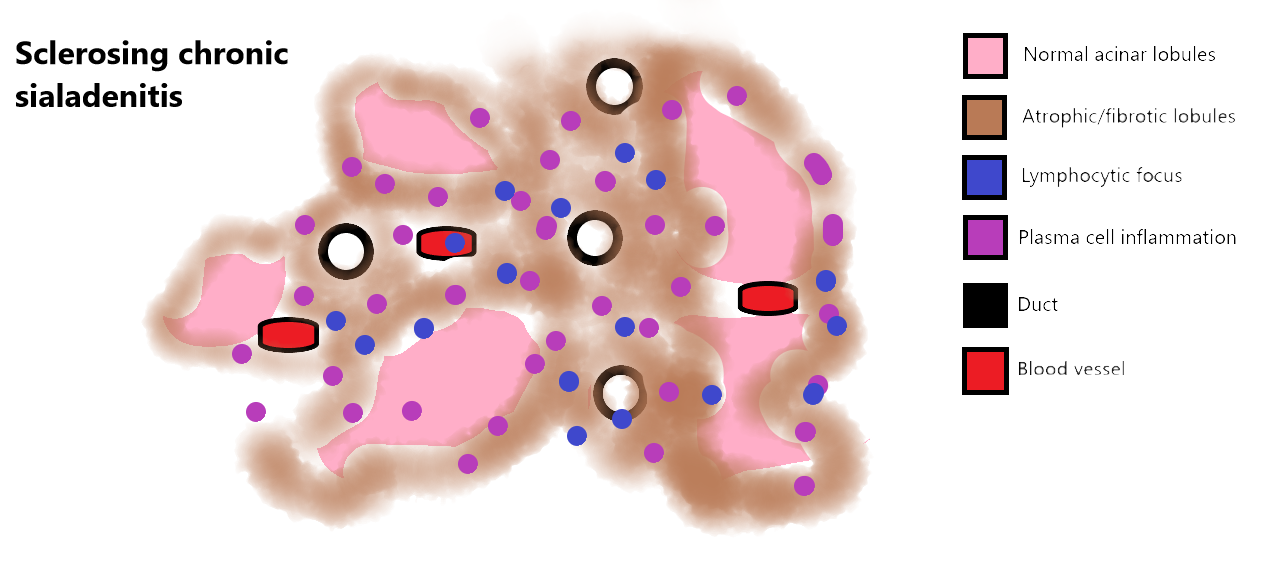
Lymphocytic Inflammation
Additional biopsy findings
Focus Score
Use this for NSCS or SCS
Final Diagnoses
Appropriate diagnoses will be highlighted based on focus score calculation or morphologic assessment
Copy to Clipboard
Copy to Clipboard
Copy to Clipboard